Understanding FASD
")
Fetal Alcohol Spectrum Disorder (FASD) is a diagnostic term used to describe the risks to the brain and body of individuals prenatally exposed to alcohol. FASD is a lifelong disability.
In the absence of appropriate interventions and support, challenges across the lifespan can lead to difficulties in employment, experience trouble with the police, mental health problems, substance misuse, and other equally serious complications.

Guide to the FASD diagnosis
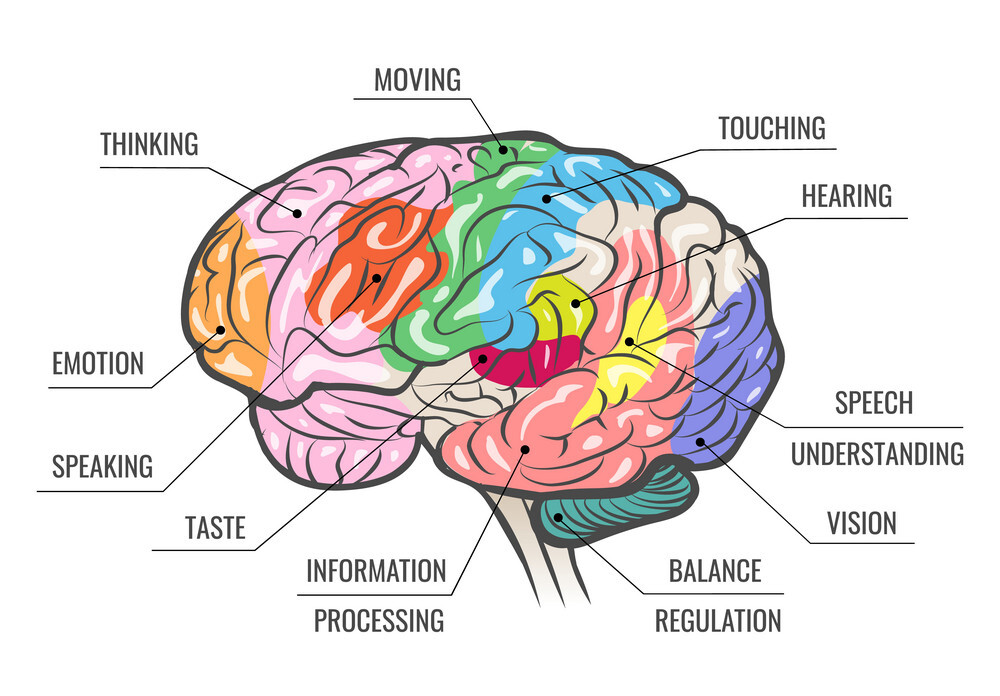
The parts of the brain most commonly affected are:

Hypothalamus
Temperature, thirst, hunger, sleep, mood, sex drive;

Hippocampus
Emotions, memory, spatial function;

Amygdala
Emotions, survival, memory

Corpus callosum
Connects the two hemispheres, motor, sensory, cognitive performances;

Frontal lobe
Executive function – the higher order thinking, problem-solving and decision-making
More typical characteristics of FASD
If you suspect that an individual in your care or who you support, regardless of their age, may be living with undiagnosed FASD, gather all the information you can find and take it to your GP. A diagnosis can only be made by your doctor or a team of specialists.
Dysmaturity
Adaptive skills
Motor Skills
These are the specific movements of the body’s muscles to perform small or large tasks and can include writing, picking up small items or walking, running or riding a bike (balance). The brain and muscles have to work together.
Sensory systems
Nutrition
Adverse reactions to different food types.
Communication and processing pace
Dependent on how fast the brain processes information, the individual living with FASD may talk excessively and quickly; interrupt others; find it difficult to join in topics of conversation; seem opinionated; make inappropriate comments or comments not in context with conversation; and repeat statements frequently.
Learning and memory
Abstract thinking
difficulty organising and managing daily tasks; struggles to manage money or time and follow through on multi-step instructions.
Executive functioning
Unable to plan and follow through with task and difficulty is more evident with more complex tasks. Concrete thinking is evident.
Strengths:
If you suspect that an individual in your care or who you support, regardless of their age, may be living with undiagnosed FASD, gather all the information you can find and take it to your GP. A diagnosis can only be made by your doctor or a team of specialists.
Behaviour is mislabelled and not understood as symptomatic of brain difference. Regulation of actions can be difficult
- Poor anger management
- Fearless in the face of danger
- Impulsive and compulsive
- Perseverative
- Inattentive [often diagnosed or mis-diagnosed as ADHD | ADD
- Unusual activity level [high or low]
- Lying
- Stealing
- Unusual reactivity to sound, touch, light
- Fidgety, cannot sit still
It is estimated that approximately 10% of children exposed to alcohol during pregnancy will have physical signs of FASD. Such individuals may be shorter and/or thinner than other children the same age, in effect, a smaller stature for age. They may have wide-spaced eyes with slanted or droopy eyelids; and the distance between the upper lip and nose may be long and/or there may be a smooth space (philtrum) with a thin vermillion border (upper lip).





